
Clinical workflow in healthcare is the backbone of every patient interaction inside a hospital. It determines how fast a patient moves from intake to diagnosis, how accurately information transfers between care teams, how completely a record is documented before it reaches billing, and how quickly a decision gets made when one is needed. When it works, the entire facility moves with it. When it breaks, everything downstream breaks with it.
And it is breaking. Not randomly, but at the same seven points, across hospitals of every size and funding level. The consequences are measurable. According to data from the Journal of Patient Safety and Johns Hopkins research, nearly 30% of medical malpractice cases in the U.S. are linked to communication and workflow failures, contributing to billions in costs annually and thousands of preventable deaths.
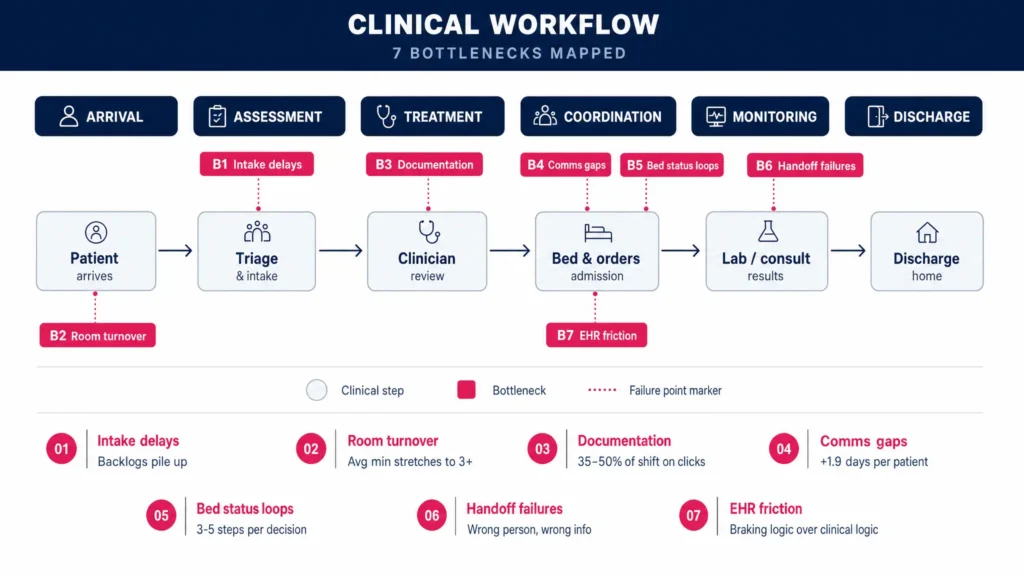
Here is where each of those seven bottlenecks lives, what it costs, and how AI is eliminating it in hospitals running right now.
What Is Clinical Workflow in Healthcare?
Clinical workflow in healthcare is the complete sequence of coordinated steps a care team follows to move a patient from arrival through treatment to discharge, and every step depends on the one before it.
Four distinct workflow types run simultaneously inside any hospital. Inter-organisational workflows govern how information moves between separate entities such as a referring physician and an emergency department. Clinical-level workflows cover the movement of information within a practice between nurses, doctors, and patients. Intra-visit workflows define the specific protocols followed during a single patient consultation. Cognitive workflows represent the decision-making process inside a clinician’s mind.
When any one of these layers breaks, the other three absorb the cost. A communication gap delays a bed status decision. A delayed bed decision extends length of stay. An extended length of stay reduces availability for the next patient. This is why healthcare process improvement cannot treat these layers in isolation. The system fails or succeeds as a whole.
7 Clinical Workflow Bottlenecks and the AI Solutions Fixing Them
These seven failure points show up not on dashboards, but in denial rates, resignation letters, and patient complaints.
| # | Bottleneck | What It Costs You |
| 01 | Patient intake delays | Backlogs form before any clinical decision is made. AI intake automation cuts this at the source |
| 02 | Inefficient room turnover | A 45-minute bed turn stretches to 2 hours without real-time visibility |
| 03 | Documentation burden | Clinicians spend 35 to 50% of their shift charting. NLP clinical notes automation changes this structurally |
| 04 | Communication gaps | Late pages and scheduling friction add an average of 1.8 days per patient stay |
| 05 | Bed status decision loops | One admission decision cycles through 3 to 5 departments. Prior authorization delays extend it further |
| 06 | Inter-department handoff failures | Lab results reach the wrong person and consult requests go unanswered. Systems design failures, not staff failures |
| 07 | EHR friction | Interfaces built around billing logic rather than clinical logic quietly push error rates up. EHR workflow optimization is the discipline of fixing this |
01. Patient Intake Delays
The challenge: Before a single clinical decision is made, time is already being lost. Manual check-in processes, unverified insurance details, incomplete pre-visit data, and scheduling gaps create a backlog at the very first touchpoint. Every minute lost at intake compounds into longer wait times, delayed triage decisions, and a poor first impression before a patient has seen a single clinician. Healthcare process improvement efforts that skip this layer never fix the downstream delays that follow from it.
Automated Patient Intake and Scheduling
AI-driven patient intake automation eliminates the manual bottleneck before the patient walks through the door:
- Pre-visit data collection is handled automatically, capturing insurance details, medical history, and consent forms digitally before the appointment date
- Eligibility verification runs in real time so coverage gaps are identified and resolved before the patient arrives, not during check-in
- Scheduling optimisation uses AI to fill gaps, reduce no-shows, and match appointment types to the right clinical resources automatically
- Triage preparation ensures the care team has complete patient context before the first interaction, removing the back-and-forth that delays the clinical handoff
02. Inefficient Room Turnover
The challenge: Without real-time visibility into bed availability, patient location, and equipment status, staff spend their shifts locating resources rather than moving patients through care. A bed that should turn over in 45 minutes sits occupied for two hours because no one has a clear picture of its status. That delay does not stay in one room. It ripples across every department waiting on that bed, directly extending length of stay for patients already in the queue.
Real-Time Location and Bed Management
AI-powered bed management and RTLS give clinical teams the visibility they need to turn rooms faster and move patients through without manual status checks:
- Live bed status dashboards show every bed across the facility in real time, eliminating radio calls and manual updates between nursing and housekeeping teams
- Automated turnover alerts notify the cleaning and prep team the moment a patient is discharged, reducing the gap between discharge and the next admission
- Equipment tracking locates wheelchairs, IV pumps, and portable devices instantly so staff stop losing time searching for resources already in the building
- Predictive occupancy modelling anticipates bed demand by shift and flags capacity pressure before it becomes a bottleneck, giving administrators time to act rather than react
03. Documentation Burden
The challenge: Clinicians spend between 35 and 50% of their shift on documentation. That figure has barely moved despite multiple EHR upgrades. The problem is structural, not behavioural. Clinical notes are being written after the fact, from memory, in interfaces built around billing requirements rather than clinical logic. The result is fragmented attention during consultations, incomplete records at the point of care, and a documentation backlog that follows clinicians beyond their shift hours. Clinical documentation improvement at this layer is not a compliance initiative. It is one of the highest-leverage operational changes a hospital can make.
Ambient Clinical Documentation Powered by NLP
Ambient clinical documentation changes the model entirely by removing documentation as a separate task:
- Real-time note generation captures the clinical conversation as it happens and structures it into a complete note without the clinician typing a single line during the visit
- Specialty-specific templates ensure the AI generates documentation that matches the format and requirements of each clinical discipline without manual adjustment
- EHR integration pushes the completed note directly into the patient record within the existing system so there is no additional platform for clinicians to navigate
- Review and approval workflow presents the clinician with a structured, accurate draft at the end of the visit rather than a blank field, reducing authoring time to minutes
04. Communication Gaps Between Care Teams
The challenge: A study of 316 patients found more than 50 delays caused by consultation and procedure scheduling. The average delay added 1.8 days to each patient’s length of stay. The two leading causes were late responses to pages and scheduling difficulties between departments. Hospitals running on pagers, personal phones, and general-purpose messaging apps are operating clinical communication on infrastructure that was never designed for it and was never built to maintain a complete, auditable record of what was said, by whom, and when.
HIPAA-Compliant AI Communication Platforms
Purpose-built clinical communication platforms replace fragmented infrastructure with a single, secure, role-based system:
- Role-based messaging ensures every consult request, lab result notification, and care update reaches the right clinician directly rather than sitting in a general inbox or going to an unavailable pager
- Automated escalation detects unanswered requests and routes them to the next available team member after a defined threshold, removing the manual follow-up loop
- Audit trails maintain a complete timestamped record of every clinical communication, supporting compliance requirements and reducing medico-legal exposure
- Integration with scheduling systems surfaces clinician availability before a consult request is sent, reducing the back-and-forth that delays specialist input and extends patient stays
05. Bed Status Decision Loops
The challenge: A single admission decision can involve an admitting physician, a hospitalist, a utilization review team, a peer-to-peer review process, and a revenue cycle team. That is three to five departments cycling through one clinical call before a bed is assigned. Prior authorization delays sit inside this same loop and extend it further, adding payer-side friction to an already crowded decision chain. The patient waits. The bed sits. The downstream schedule shifts.
AI Clinical Decision Support at the Point of Care
AI clinical decision support embeds the information needed to make admission decisions directly inside the EHR at the moment a physician needs it, collapsing a multi-department loop into a single documented call:
- Admission criteria surfacing presents the relevant clinical guidelines and payer requirements inside the EHR in real time so the physician has everything needed to make the decision without consulting a separate system
- Prior authorization automation identifies authorisation requirements, prepares the supporting documentation, and submits to the payer without manual preparation by the clinical or RCM team
- Peer-to-peer scheduling support flags cases likely to require peer review early in the process and prepares the clinical summary in advance, reducing preparation time when the call is scheduled
- Decision audit trails document the clinical rationale for each admission decision inside the patient record, supporting compliance and reducing the back-and-forth with utilization review teams
Fix the Decision Loop Before It Costs You Another Bed
AI puts the right clinical information in front of the right physician at the right moment.
06. Inter-Department Handoff Failures
The challenge: Information lost between specialists, labs, imaging teams, and the primary care team is one of the most common and least discussed sources of clinical error. Consult requests sit unanswered. Lab results reach the wrong recipient. Imaging reports do not transfer cleanly between systems. These are not failures caused by careless staff. They are failures caused by systems that were never designed to move structured clinical information reliably across departments operating on different platforms and different schedules. Clinical workflow solutions that do not address the handoff layer leave one of the highest-risk gaps in the entire care journey unresolved.
Automated Handoff and Clinical Data Exchange
AI-powered handoff workflows and integrated clinical data exchange eliminate the gaps that form between departments:
- Structured handoff protocols standardise what information transfers at each clinical transition point so nothing is left to verbal summary or individual memory
- Automated result routing sends lab results, imaging reports, and pathology findings directly to the responsible clinician with a read-receipt confirmation, removing the assumption that delivery equals receipt
- Cross-system data reconciliation ensures patient records remain consistent across departments, specialties, and facilities even when each operates on a different EHR instance or platform
- Handoff tracking dashboards give charge nurses and department leads a real-time view of every pending handoff, flagging delays before they become clinical risks
07. EHR Friction and Poor Interface Design
The challenge: A poorly designed EHR interface does more damage than most administrators realise. Slow data entry, non-intuitive navigation, and interfaces built around billing logic rather than clinical logic all increase cognitive load and quietly push error rates up. Clinicians develop workarounds. Workarounds introduce inconsistency. Inconsistency produces incomplete records that generate claim denials and compliance exposure. EHR workflow optimization is the discipline of making clinical software work the way clinicians actually think, and most hospitals have not invested in it seriously yet.
EHR Workflow Optimization and Interface Redesign
Redesigning the EHR around clinical logic rather than billing logic removes friction at every step of the documentation process:
- Clinical logic mapping audits the current EHR interface against the actual steps a clinician follows during a consultation and identifies every point where the interface adds friction rather than reducing it
- Role-specific views configure the EHR display to show each user only the information relevant to their function, reducing the cognitive load of navigating screens built for a different role
- Workflow automation within the EHR handles repetitive data entry, auto-populates fields from existing patient data, and reduces the number of clicks required to complete a standard documentation task
- Continuous performance monitoring tracks where documentation lags, where workarounds cluster, and where error rates are highest so optimization is an ongoing process rather than a one-time implementation project
How CaliberFocus Approaches Clinical Workflow in Healthcare Differently
Most clinical workflow solutions automate individual tasks. CaliberFocus builds autonomous agents that make decisions across the entire workflow without waiting for human intervention at every step.
The difference is not incremental. A traditional automation tool flags a denied claim and waits for a staff member to act. A CaliberFocus autonomous agent identifies the denial pattern, pulls the relevant clinical documentation, builds the appeal, and routes it to the payer without a single manual touchpoint in between.
This distinction matters across every layer of clinical workflow in healthcare:
- At the documentation layer, autonomous agents capture, structure, and validate clinical notes in real time rather than prompting clinicians to complete them after the fact
- At the revenue cycle layer, agents handle claims processing, denial recovery, and payer communication end to end rather than flagging exceptions for staff to resolve manually
- At the decision support layer, agents surface admission criteria, prior authorization requirements, and clinical guidance inside the EHR at the exact moment a physician needs them
- At the communication layer, AI voice agents manage payer follow-up calls, status checks, and appeal submissions without consuming RCM staff hours
What CaliberFocus delivers is not a faster version of the workflow your team is already running. It is a redesigned one where autonomous intelligence handles the repeatable, rule-based, and call-intensive work so your clinical and revenue cycle teams focus entirely on what requires human judgement.
If your hospital is absorbing avoidable delays, rising denial rates, or documentation overload that your current tools have not solved, the next step is a conversation about where autonomous agents fit into your specific workflow.
Scale your business with AI innovation
Build intelligent systems using generative AI, automation, and machine learning solutions designed for modern enterprises.
Frequently Asked Questions
Traditional healthcare process improvement redesigns processes and retrains staff. Clinical workflow automation deploys AI agents that actively execute steps, from documentation capture to claims submission to payer follow-up, without human intervention at each stage. Repeatable tasks are handled autonomously so clinical staff focus on decisions that require human judgement.
Ambient clinical documentation removes documentation as a separate task. The AI captures and structures the clinical note in real time during the consultation. The clinician reviews and approves at the end rather than charting from scratch. This returns hours per shift to clinicians and produces more complete records that reduce downstream claim denials.
AI clinical decision support surfaces admission criteria and prior authorization requirements inside the EHR before a physician makes a decision. Decisions made with complete information generate accurate, submission-ready documentation. That accuracy reduces claim denials and shortens appeal cycles without additional RCM effort.
Yes. Clinical workflow solutions that operate across the full patient journey create compounding improvements. Accurate documentation produces cleaner claims. Cleaner claims reduce denial rates. Lower denial rates reduce RCM recovery hours. EHR workflow optimization at the clinical layer has a direct and measurable effect on the financial layer.
The key distinction is whether a solution automates isolated tasks or operates across a connected workflow. AI in healthcare operations delivers ROI when it handles the full sequence of a process, not just one step. Look for demonstrated outcomes in length-of-stay reduction, denial rate improvement, and clinician hours returned per shift.