
Medical billing denials are rarely random. Most organizations already know the common codes appearing across their remittance files. The challenge is not identifying them. The challenge is reducing them consistently without adding more manual review, more spreadsheets, or more rework cycles.
That is why denial management in medical billing is shifting from reactive correction toward proactive prevention.
The most common denials including eligibility failures, prior authorization gaps, coding issues, duplicate submissions, medical necessity denial, and timely filing problems originate before the claim reaches the payer. When those signals are identified early, denial prevention becomes operational rather than administrative.This is where AI changes the workflow. Instead of detecting issues after an EOB explanation of benefits denial or electronic remittance advice ERA arrives, intelligence operates across eligibility verification, clinical documentation, coding validation, claim processing, and prevention workflows to identify risk before submission. This shift is becoming foundational to organizations adopting AI agents for denial management.
Your Team Already Knows the Denials. The Problem Is the Denial Management Workflow.
The cycle usually looks like this:
Claim submitted → Payer adjudication → Denial returned → Team investigates → Appeal submitted → Revenue delayed
Across healthcare organizations, the majority of denied claims repeatedly fall into the same categories.
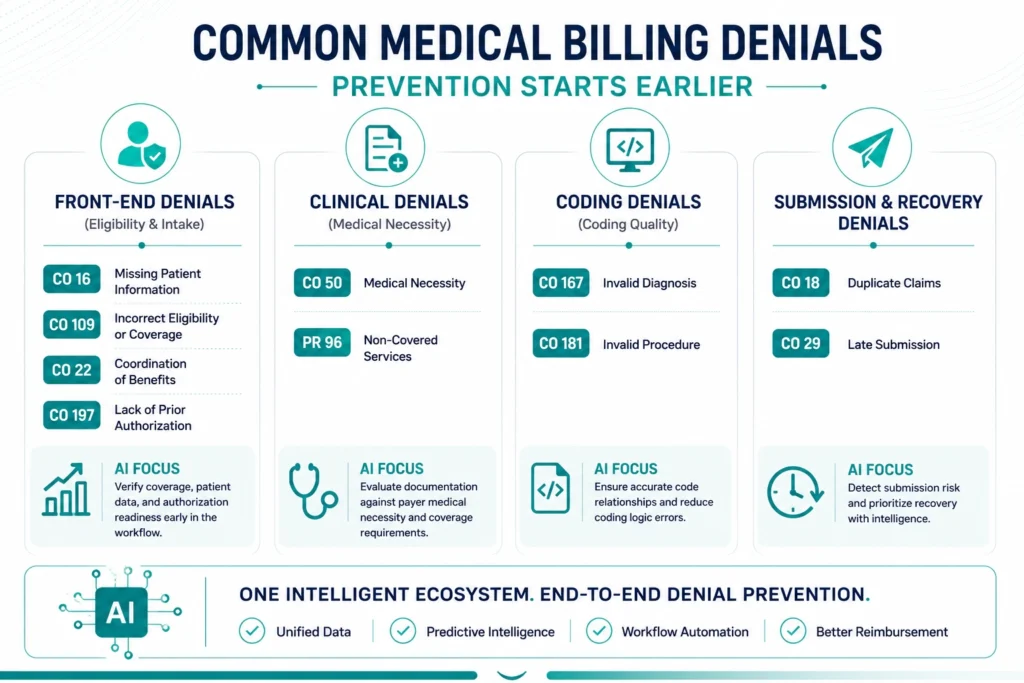
| Common Medical Billing Denial | Denial Code |
| Missing or Incomplete Patient Information | CO-16 |
| Incorrect Patient Eligibility or Coverage | CO-109 |
| Duplicate Claims | CO-18 |
| Lack of Prior Authorization | CO-197 |
| Invalid or Unsupported Diagnosis Code | CO-167 |
| Invalid or Unsupported Procedure Code | CO-181 |
| Non-Covered Services | PR-96 |
| Medical Necessity Denials | CO-50 |
| Late Claim Submission | CO-29 |
| Coordination of Benefits Errors | CO-22 |
These denials appear across different stages of the revenue cycle, but they rarely happen in isolation. Most originate from eligibility gaps, missing authorization steps, documentation and coding misalignment, submission risk, or coverage validation failures.
That is why denial management in medical billing often becomes reactive even when teams already know which denial codes continue appearing.
The opportunity is not faster recovery. The opportunity is proactive denial prevention by identifying and intercepting the conditions that create denials before submission.
Each denial category above has a different intervention point.
The sections below map those common denials to the AI capabilities that realistically reduce them.
Front-End Denials: Where AI Prevents Errors Before Claims Exist
Many high-volume denials begin before care delivery starts.
These denials are commonly tied to patient intake, insurance eligibility verification, authorization workflows, and coordination of benefits.
| Denial | Why It Happens | AI Prevention Layer |
| CO-16 denial code medical billing | Missing or invalid patient information | Eligibility validation intelligence |
| CO-109 | Coverage inactive on date of service | Real-time eligibility monitoring |
| CO-22 | Coordination of benefits issues | Coverage sequencing validation |
| Prior authorization denial | Authorization missing or mismatched | Prior authorization workflow intelligence |
Traditional workflows validate eligibility at check-in.
AI-enabled workflows validate continuously from scheduling through the date of service.
Eligibility Verification Intelligence
Eligibility intelligence combines payer data, patient intake, and workflow orchestration to validate:
- Active policy status
- Subscriber consistency
- Coordination of benefits
- Service eligibility
- Coverage changes before appointment date
Organizations expanding insurance eligibility verification are increasingly adopting AI agents for eligibility verification to identify coverage risk before the encounter becomes a claim.
Prior Authorization Intelligence
Prior authorization denial rarely happens because teams ignore process.
It usually happens because authorization logic changes across payer and procedure combinations.
AI coordinates:
- Procedure-level authorization requirements
- Authorization validity windows
- Documentation completeness
- Procedure mismatch detection
This is one reason many RCM organizations are investing in prior authorization AI to automate authorization identification and tracking.
Clinical Denials: Why Medical Necessity Cannot Be Solved by Rules Alone
Medical necessity denial categories represent one of the highest-value revenue leakage points in revenue cycle operations.
This includes:
- CO-50 denial code
- Invalid diagnosis scenarios
- Procedure justification failures
- CARC codes medical billing patterns
- Documentation gaps
These denials are often treated as coding problems.
In practice, they begin earlier.
Step 1: Clinical Documentation Understanding
Through AI agents for clinical documentation, NLP interprets clinical records and extracts reimbursement-relevant indicators.
That includes:
- Symptoms
- Severity indicators
- Treatment progression
- Clinical evidence
- Encounter context
Step 2: Documentation-to-Payer Validation
After extracting clinical indicators, the intelligence layer evaluates whether the documented encounter aligns with the payer’s active reimbursement and medical necessity criteria.
This validation considers:
- Procedure-specific payer requirements
- Diagnosis and treatment alignment
- Coverage and medical necessity conditions
- Documentation sufficiency for reimbursement review
When gaps appear, the claim is flagged before final coding and submission so teams can resolve documentation issues earlier in the workflow.
The objective is not to predict payment. The objective is to identify reimbursement risk before the claim reaches adjudication.
Step 3: Predictive Denial Scoring
Before submission, predictive intelligence evaluates:
- Historical payer outcomes
- ICD and CPT combinations
- Procedure risk
- Provider-level denial trends
High-risk claims are surfaced before they become appeals.
Combined with AI in medical billing and coding and data analytics in medical coding, denial prevention becomes proactive validation instead of retrospective correction.
A CO-50 denial does not begin inside billing. It begins when documentation and reimbursement requirements are never evaluated together.
Operationalize denial prevention across RCM
Create earlier intervention points across eligibility, documentation, and claims workflows.
Submission Denials: Why Existing Claim Scrubbing Still Misses Revenue
Many organizations assume clearinghouse medical billing processes eliminate submission risk.
That assumption creates blind spots.
CO-11 and CO-97: Coding and Bundling Logic
Traditional scrubbers apply broad edit logic.
AI evaluates:
- Modifier relationships
- Historical payer patterns
- Service combinations
- Coding sequence risk
Duplicate Claim Denial (CO-18)
Duplicate claim denial is rarely an exact duplicate.
Machine learning identifies semantic similarity across:
- Encounter history
- Claim timing
- Service overlap
- Submission patterns
Timely Filing Denial (CO-29)
Calendar reminders do not prioritize claim urgency.
Workflow intelligence reorganizes submission queues using:
- Filing deadlines
- Revenue impact
- Claim aging
- Submission windows
Supported through AI agents for claim processing, these workflows help reduce preventable denial accumulation.
PR Denial Codes and Non-Covered Services
PR denial codes often appear after services have already been delivered and reimbursement responsibility shifts to the patient.
A common assumption is that eligibility verification prevents these denials.
In practice, eligibility only confirms that the policy is active. Coverage intelligence evaluates whether the specific service, procedure, frequency limits, medical policy conditions, and benefit rules qualify for reimbursement under that patient’s plan.
This distinction matters because a patient can be eligible for insurance and still receive a non-covered service.
AI helps identify these coverage risks earlier by evaluating benefit conditions and payer requirements before submission rather than after denial.
Not All Denials Need the Same AI
One AI agent cannot realistically solve every denial category.
Different denials require different intelligence layers because each failure originates at a different decision point across the revenue cycle.
| Denial Category | How AI Prevents the Denial |
| Eligibility and intake | Detects inactive coverage, missing subscriber information, and coordination mismatches before scheduling or registration turns into a billable encounter |
| Authorization | Matches procedures against payer authorization rules, tracks approval validity windows, and prevents claims from entering submission without authorization readiness |
| Medical necessity | Connects clinical documentation with diagnosis and payer policy requirements to identify insufficient justification before reimbursement review |
| Coding quality | Evaluates diagnosis, procedure, modifier, and encounter relationships to reduce unsupported coding combinations and payer edit failures |
| Submission risk | Identifies duplicate claims, filing deadline exposure, and historical payer denial patterns to prevent avoidable claim rejection and rework |
| AR recovery | Prioritizes denial queues based on reimbursement probability, prepares recovery actions, and shortens manual appeal and follow-up cycles |
The practical architecture is orchestration.
Organizations moving toward enterprise-scale prevention are increasingly adopting agentic AI workflows for healthcare RCM so teams manage exceptions instead of repetitive validation.
What Changes When AI Operates Before Submission
When denial prevention becomes embedded into the revenue cycle, the biggest shift is not fewer denials.
The shift is that revenue cycle teams stop operating in recovery mode.
| Traditional Denial Management | AI-Driven Denial Prevention |
| Teams discover issues after payer adjudication | Teams identify reimbursement risk before submission |
| Eligibility and authorization are checked once | Validation continues throughout the claim lifecycle |
| Coding and documentation are reviewed independently | Clinical, coding, and payer signals are evaluated together |
| Claims move through standard queues | Submission is prioritized based on denial probability |
| AR teams spend time recovering preventable denials | Recovery efforts focus on high-value and complex claims |
| Operational reporting explains what happened | Predictive workflows influence what happens next |
For RCM leaders, this changes how performance improves.
Higher first pass claim rates become a result of earlier decisions.
Cleaner claims become an output of continuous validation.
Accounts receivable teams spend less time fixing avoidable issues and more time accelerating reimbursement.
This approach improves operational efficiency without replacing billing expertise. It shifts expertise toward exception handling, payer strategy, and revenue optimization.
How healthcare organizations move from denial recovery to prevention
Read how AI agents helped improve revenue cycle workflows by reducing manual intervention and enabling earlier reimbursement decisions.
Frequently Asked Questions
Recurring medical billing denial codes usually indicate that validation is happening too late in the denial management workflow. Teams improve recovery processes but continue allowing eligibility gaps, prior authorization issues, documentation gaps, and submission risk to enter the claim lifecycle. Sustainable reduction requires proactive denial prevention before claims reach adjudication.
Not with one decision model.
Different categories of revenue cycle management denials require different intelligence layers because each failure originates at a different point in the workflow. Eligibility failures require insurance eligibility verification, medical necessity denial requires clinical reasoning, and duplicate claim denial requires predictive submission controls.
The most effective approach connects specialized AI capabilities through orchestration instead of relying on standalone denial management software.
AI evaluates clinical documentation before coding begins, extracts reimbursement signals from clinical notes, and compares them against payer-specific medical necessity criteria.
Claims with insufficient support are identified before submission, reducing CO-50 denial code exposure and improving first pass claim rate through earlier intervention.
Software centralizes claims denial management activity but does not automatically reduce denials.
Improving first pass claim rate and achieving measurable clean claim rate improvement usually requires intelligence embedded into insurance eligibility verification, coding validation, authorization workflows, and submission decisions before claims enter the payer cycle.
AI supports the insurance denial appeal process by prioritizing denied claims, organizing supporting evidence, automating follow-up workflows, and improving visibility across accounts receivable denial management.
This allows billing teams to reduce manual recovery effort and focus on high-value reimbursement decisions instead of repetitive outreach.
AI contributes to denial prevention in medical coding by flagging high-risk codes using historical denial data, payer patterns, and coding validation signals before claims are submitted. Instead of replacing coders or assigning final codes independently, AI helps identify reimbursement risk early by evaluating diagnosis and procedure combinations, historical payer outcomes, documentation alignment, and coding patterns that commonly lead to denials. This enables teams to resolve issues proactively and improve clean claim and first-pass claim performance.
Extend denial prevention across the revenue cycle
Apply AI across eligibility, documentation, coding, claims, and reimbursement workflows to improve revenue cycle performance.
Learn About AI Agents for RCM →