")
Hospital operations bleed efficiency across gaps most teams can see but can’t fix at scale, a discharge flagged at 11 AM, a bed idle through the morning shift, an ED patient waiting downstream. On the revenue cycle side, that same delayed information compounds further: 5–10% of claims return denied, half of those never get resubmitted, and prior authorization turnaround runs 3–7 days while the procedures those admits generated sit on hold.
Both share the same root cause, manual workflows operating on delayed, incomplete information.
AI in healthcare operations addresses this directly. Predictive models surface discharge readiness hours in advance. NLP tools reduce physician documentation time by 50–70% per encounter. AI agents validate claims before submission, handle prior auth tracking without staff follow-up, and prioritize denial queues by recovery value, pulling Days in A/R from the 45–60 day range down to 28–38.
Health systems deploying AI against the right workflows first are seeing denial rates drop from 10% to under 5% and ED boarding time fall by 15–25%.
Your Operations Are Generating Signals. Are You Acting on Them?
CaliberFocus helps you build the AI infrastructure to close them in the right sequence.
Where Healthcare Operations Actually Lose Ground
Healthcare facilities run on interdependent systems: clinical, administrative, and financial. A delay in one cascades across the others. A bed not turned on time, a prior authorization stalling for four days, a shift running understaffed because census forecasts were off. Each carries a direct downstream financial consequence that most organizations track at the aggregate level but rarely at the decision point where it could be prevented.
The operational gaps are rarely invisible. Hospital administrators know which units routinely run over capacity, which payer mixes generate the most denials, and which shifts consistently run short. What most lack is the infrastructure to act on that knowledge before the cost is already incurred. AI in healthcare operations closes that gap, surfacing signals early enough for decisions to change outcomes.
1. Administrative Automation
Administrative tasks account for an estimated 30–35% of total US healthcare spend, a figure that hasn’t improved meaningfully despite decades of EHR investment. The burden sits predominantly on clinical staff: physicians logging two hours of documentation for every hour of direct patient care, billing teams managing eligibility verification and coding simultaneously, and registration workflows built for far lower patient volumes than most facilities now handle.
Healthcare automation tools deployed at this layer address each of these systematically.
- NLP-driven EHR transcription captures physician-patient conversations and converts them into structured clinical notes in real time, with no manual dictation or post-encounter entry required. NLP in clinical documentation removes documentation errors before they enter the workflow, cutting downstream coding issues at the source. Physicians reclaim session capacity without extending hours.
- AI patient scheduling systems predict appointment duration from visit type and patient history, flag high no-show risk 48–72 hours ahead, and route referrals to the right specialist slot automatically. AI chatbots for appointment scheduling and patient triage extend this into triage-level decisions, handling volume that front-desk staff cannot absorb at scale.
- Patient intake automation structures demographic, insurance, and clinical history data at the first touchpoint, feeding accurate inputs into scheduling, eligibility verification, and care planning downstream. Upstream errors caught here don’t surface later as claim denials. AI patient intake in healthcare operations covers how this reduces registration-stage gaps that compound in the revenue cycle.
For teams assessing existing EHR infrastructure before adding automation, best practices for automating EHR processes covers the integration decisions that determine whether this layer performs or creates new technical debt.
2. Patient Flow and Capacity Management
ED overcrowding, extended boarding times, and delayed elective procedures share a common operational pattern: the response happens after the bottleneck has formed. Capacity decisions made in real time, against demand that has already exceeded available resources, produce outcomes that are predictable and largely preventable.
Predictive AI for patient flow changes the decision window. Admission forecasting models pull from historical census data, seasonal trends, and real-time ED acuity to project unit-level demand 12–24 hours ahead. Bed management teams receive that projection before the shift, with enough lead time to act. Discharge readiness is flagged from care plan data, medication completion, pending labs, transport requirements, typically 4–6 hours before the care team would otherwise identify it. Housekeeping, case management, and the receiving unit prepare simultaneously, compressing the actual bed turnover window in a way sequential handoffs never allow.
At the ED level, predictive models monitor patient flow against historical diversion triggers, surfacing early warning signals before boarding escalates. Health systems with mature patient flow AI report 15–25% reductions in ED boarding time and measurable gains in elective procedure throughput.
The financial return runs in two directions. Improved throughput increases revenue-generating capacity without adding beds. Proactive discharge management reduces observation-to-admission conversion rates that payers are increasingly scrutinizing under value-based care models. Predictive analytics in healthcare covers the data infrastructure required to make these forecasts accurate and operationally reliable at scale.
3. Workforce Planning and Staffing AI
Replacing a single bedside RN, when agency coverage, onboarding, and lost productivity are included, costs between $40,000 and $60,000. Most health systems absorb this cost repeatedly, across multiple departments, every quarter, because staffing decisions are built on last month’s census data rather than forward-looking demand models.
AI-powered staff rostering integrates patient census forecasts, shift-level demand history, skill mix requirements, and overtime thresholds to build schedules that maintain safe nurse-to-patient ratios while reducing agency dependency. Across health systems that have deployed it, the measurable impact includes:
- Labor cost variance reduced by 10–20% through demand-based scheduling calibrated to actual census
- Float pool utilization optimized, reducing premium-rate agency calls during predictable surge periods
- Schedule unpredictability reduced, a direct driver of nursing attrition that overtime cost calculations rarely capture
- Overtime spend compressed from the 12–18% of total labor cost range toward 6–9%
The retention benefit is consistently underweighted in ROI projections. Medscape’s 2024 burnout report places physician burnout at 48%, with documentation burden and schedule unpredictability among the primary drivers. AI addresses both. How AI helps healthcare overcome staffing shortages covers the near-term operational playbook for facilities managing active gaps.
Health systems that measure staffing AI only against overtime savings miss the retention dynamic. Reducing department-level churn produces financial returns that consistently exceed what labor cost reduction alone delivers.
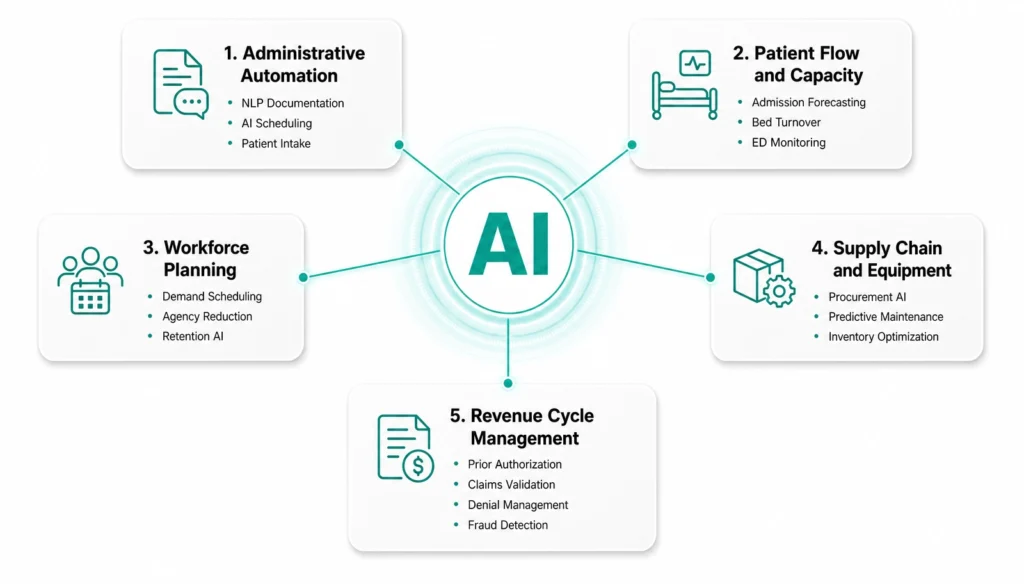
4. Supply Chain and Equipment
A surgical center carrying 60 days of inventory for high-cost orthopedic implants is absorbing carrying costs that could fund two additional FTEs. A facility that runs short on a critical surgical supply Monday morning delays procedures that took weeks to schedule. Both outcomes live within the same supply chain and share the same root cause: procurement decisions built on historical averages, with no visibility into actual upcoming procedure demand.
Pharmaceutical and Surgical Supply Management
AI monitors usage rates, expiry timelines, and procedure schedules continuously, generating automated purchase orders calibrated to real demand. Integration with EHR procedure schedules means the system identifies a high-volume orthopedic block before the supply manager does and adjusts orders accordingly. Facilities managing this manually report surgical supply waste from near-expiry inventory in the 15–25% range. How AI streamlines procurement in healthcare facilities covers the workflow model that makes this operationally sustainable across multiple service lines and locations.
Clinical Equipment and Predictive Maintenance
AI for medical equipment maintenance uses IoT sensor data from MRI scanners, infusion pumps, and ventilators to identify failure patterns before a breakdown occurs. A single unplanned MRI outage displaces 30–50 scans and creates scheduling disruption that compounds for days across dependent workflows. Predictive maintenance shifts the cost from emergency repair and procedure displacement to planned downtime scheduled during low-utilization windows. For facilities running high-value diagnostic equipment across multiple sites, the financial case closes faster than most capital planning cycles anticipate.
5. Revenue Cycle AI
Revenue cycle management has more AI deployed against it than any other healthcare operational function, yet denial rates hold at 5–10%, Days in A/R average 45–60 days, and prior authorization turnaround continues to stall scheduled procedures for 3–7 days. Most organizations have automated individual steps in the cycle. The gaps compound in the handoffs between them, and that’s where the financial leakage persists.
AI-driven revenue cycle management closes this by operating across the complete financial workflow, with autonomous agents handling multi-step tasks end to end.
- Prior authorization: Prior authorization AI agents submit requests, track payer responses, escalate stalled cases, and format appeals to exact payer specifications. Turnaround compresses from 3–7 days to same-day in mature implementations, removing the single largest scheduling bottleneck in most health systems.
- Claims validation: AI validates CPT and ICD-10 codes against payer-specific rules before submission and runs eligibility verification at the scheduling stage rather than at the billing stage. AI in medical billing and coding covers the coding compliance model that improves first-pass acceptance rates before a claim leaves the system.
- Denial management: AI agents for denial management categorize denials by root cause, prioritize by dollar value, and route or resolve autonomously. The 50–60% of denied claims that are never resubmitted under manual workflows get systematically recovered.
- Fraud detection: AI in healthcare fraud detection screens every claim against known billing anomaly patterns, duplicate NPI flags, and statistically improbable procedure volumes. A manual audit team covers under 5% of claims at best. AI covers all of them, continuously.
- Payment variance: Automated detection flags underpayments against contracted rates in real time, recovering revenue that high-volume payer mixes would otherwise absorb quietly.
AI agents for RCM covers the agent architecture that makes full-cycle autonomous resolution possible. Health systems with complete deployment report denial rates at 3–5%, Days in A/R at 28–38 days, and prior auth turnaround at same-day.
Where to Start Based on Your Vertical
AI readiness varies significantly across healthcare. The right starting point depends on where your data lives, how mature your existing workflows are, and which operational gaps are generating the most financial drag. The framework below maps each vertical to the AI moves that produce the fastest measurable return at each stage.
Healthcare Providers
Hospital and health system operations carry the broadest AI deployment surface — patient flow, staffing, scheduling, supply chain, and clinical documentation all run in parallel and create compounding gaps when any one falls behind. The entry point is the workflow generating the most daily friction, not the most advanced use case available.
| Stage | Where You Are | First AI Move | What Changes |
| Foundation | Fragmented EHR data, manual scheduling and rostering, no real-time census visibility | AI patient scheduling + NLP-driven clinical documentation | Documentation burden drops, scheduling errors surface before they reach the floor |
| Operational | Integrated EHR, basic automation in place, some analytics capability | Predictive patient flow + AI-powered staff rostering | Bed turnover accelerates, agency utilization reduces, throughput gains become measurable |
| Predictive | Clean data infrastructure, stable RCM processes, real-time census visibility | Ambient scribing + supply chain demand forecasting | Physician capacity increases per session, surgical supply waste reduces 15–25% |
AI in hospital operations for smarter resource management covers the workflow integration model for health systems moving from foundation to operational maturity.
Payers and Health Plans
Payers manage claim volumes that manual audit workflows cannot cover at scale, fraud exposure that rule-based detection increasingly misses, and prior authorization backlogs that generate provider friction and regulatory scrutiny simultaneously. AI enters most effectively at the claims and fraud layer, then extends into member-level risk and care management.
| Stage | Where You Are | First AI Move | What Changes |
| Foundation | Rule-based fraud detection, manual prior auth review, batch claims processing | AI claims validation + fraud anomaly screening across 100% of claims | Fraud detection coverage moves from under 5% of claims to near-complete |
| Operational | Semi-automated claims adjudication, basic member analytics, some fraud detection | Prior auth automation + member risk stratification models | Auth turnaround compresses, high-risk members surface earlier in care management workflows |
| Predictive | Real-time claims processing, advanced member segmentation, predictive models in place | AI-driven care management + autonomous compliance monitoring | Preventable readmissions reduce, compliance gaps surface before audit exposure materializes |
AI agents for healthcare compliance oversight covers the regulatory monitoring layer that payers at the predictive stage deploy alongside claims AI.
Revenue Cycle Management
RCM teams running manual workflows are structurally overwhelmed at current claim volumes. Financial leakage accumulates across each handoff, eligibility at registration, prior auth at scheduling, coding at documentation, denial management post-submission. AI closes these handoffs in sequence, which is why the starting point matters more than the ambition of the deployment.
| Stage | Where You Are | First AI Move | What Changes |
| Foundation | Manual billing workflows, reactive denial management, limited EHR integration | AI denial prevention + pre-submission claims scrubbing | First-pass acceptance improves, rework volume drops within the first billing cycle |
| Operational | Integrated RCM platform, established coding team, some automation in place | AI prior auth agents + payment variance detection | Auth turnaround compresses to same-day, underpayments surface against contracted rates automatically |
| Predictive | Optimized denial workflows, stable data infrastructure, real-time A/R visibility | Full autonomous RCM agents + predictive denial analytics | Days in A/R moves from 45–60 to 28–38, denial rate drops from 10% toward 3–5% |
Agentic AI workflows for healthcare RCM covers the agent architecture that makes full-cycle autonomous resolution operationally viable across payer mixes.
Medtech and Devices
Medtech organizations carry a dual AI imperative: operational efficiency across device manufacturing and supply, and real-world performance data from devices already in the field. Both require clean data infrastructure before AI adds meaningful value. The starting point for most Medtech organizations is data capture and integration, not model deployment.
| Stage | Where You Are | First AI Move | What Changes |
| Foundation | Manual maintenance schedules, limited telemetry, basic remote monitoring capability | IoT sensor integration + predictive maintenance modeling | Unplanned device downtime reduces, emergency repair costs shift to planned maintenance windows |
| Operational | IoT-enabled devices, some predictive maintenance, basic remote monitoring in place | AI-driven real-world data capture + device anomaly detection | Performance gaps surface before field failures, post-market surveillance becomes proactive |
| Predictive | Full IoT integration, real-world data pipeline established, stable device analytics | AI-driven regulatory submission automation + performance optimization models | Submission timelines compress, device iteration cycles shorten based on real-world field evidence |
Healthcare mobile app development and remote patient monitoring covers the connected device infrastructure that feeds Medtech AI models with reliable real-world performance data.
Life Sciences and Pharma
Clinical trial data is among the most complex and highest-stakes data in healthcare, yet most life sciences organizations still manage significant portions of trial analytics manually. AI enters most productively at the data infrastructure layer first, accelerating trial timelines and surfacing the real-world evidence that regulatory submissions increasingly require before approval.
| Stage | Where You Are | First AI Move | What Changes |
| Foundation | Siloed trial data, manual regulatory submissions, basic descriptive analytics | Data integration + descriptive analytics across trial datasets | Trial data becomes queryable in real time, reporting timelines compress across study sites |
| Operational | Integrated data platforms, some automation in trial management, basic AI models in place | Predictive trial analytics + patient cohort matching AI | Trial recruitment timelines shorten, protocol deviation signals surface before they affect study outcomes |
| Predictive | Advanced real-world evidence pipeline, AI models established, regulatory AI strategy defined | Automated regulatory intelligence + AI-driven drug-target identification | Submission preparation time reduces, early-stage development cycles accelerate against defined evidence thresholds |
Big data analytics in healthcare and descriptive analytics in healthcare cover the foundational data layer life sciences organizations need before predictive models perform reliably at trial scale.
Where Does Your Health System Stand on AI Maturity?
CaliberFocus assesses your current workflows, data infrastructure, and readiness, so the deployment sequence is right from day one.
Request Your AI Maturity Assessment →How CaliberFocus Helps
Most healthcare organizations don’t have an AI problem. They have a sequencing problem, deploying AI against symptoms rather than the workflows generating them.
CaliberFocus builds AI solutions specifically for healthcare operations, covering AI-assisted medical billing and coding, end-to-end revenue cycle management, predictive denial analytics, clinical workflow automation, and AI voice agents for claim denials. Every solution is built around the operational realities health systems actually run on, not retrofitted from general-purpose tools.
Deployments that have moved coding accuracy from 87% to 98.2%, compressed Days in A/R from 45 to 29, cut denial rates by 35%, and recovered $4.2M in additional collections for a 450-provider group, without adding headcount.
The starting point is always the same: identify the right sequence before building anything.
Frequently Asked Questions
The gap is in the handoffs, not the individual steps. EHRs capture data and RCM automation processes claims, but neither predicts what is about to go wrong or acts before it does. CaliberFocus intervenes at the decision points between workflows: flagging denial-risk claims before submission, identifying prior auth gaps before they delay care, and surfacing staffing shortfalls before they impact operations. The ROI comes from closing what existing systems miss.
It is the question most vendors skip, and the reason most AI deployments underperform. Before any engagement, CaliberFocus assesses data completeness, normalization across source systems, and integration readiness. If the infrastructure needs work first, we say so. Deploying AI against fragmented data and troubleshooting accuracy six months later costs far more than getting the foundation right upfront.
AI-assisted coding, prior auth automation, and NLP-driven documentation typically deliver measurable results within 6 to 12 weeks. Full revenue cycle deployment reaches mature performance at 12 to 18 months. CaliberFocus integrates within existing EHR and billing platforms, adding capability to current workflows, not replacing them. Riverside Medical Center reached 97% coder acceptance within the first six weeks with zero workflow disruption.
For revenue cycle: first-pass claim acceptance, coding time per encounter, prior auth turnaround, and Days in A/R. For clinical operations: ED boarding time and bed turnover rate. For workforce AI: labor cost variance and agency utilization. Prior auth turnaround and clean claim rates shift within the first billing cycle. Days in A/R and denial rates reflect improvement at 90 to 180 days.
Ask for specificity in three areas. Payer rule sets, can they explain exactly how their models account for payer-specific coding requirements and denial patterns by CPT code? Compliance architecture, is HIPAA compliance built into the system or bolted on afterward? Case evidence — do they show outcomes at the workflow level: denial rate by category, coding accuracy by specialty, prior auth turnaround by payer? Aggregate ROI numbers without operational detail mean a vendor has modeled implementations, not run them.