
- The 2026 Shift: Computer-Assisted Coding Software to Autonomous Medical Coding Agents
- Why Hospitals and Health Systems Are Moving First
- Why Independent Practices and Groups Cannot Run on One Coder Anymore
- Operational Leverage: Why RCM and Billing Companies Are Scaling Without Scaling Headcount
- Trust Compliance: Why Audit Defensibility Is the Real Differentiator
- Traditional Coding Tools vs Agentic AI, Side by Side
Your coding backlog is not a staffing problem anymore. It is a structural one.
Hospitals are sitting on 10 to 45 day chart backlogs. Practices are one sick coder away from a frozen cash flow. RCM companies are quoting lower fees while clients demand faster, zero-error turnarounds. Different symptoms, same root cause: traditional coding tools assist a human, they do not replace the judgment a human has to apply chart after chart, all day, every day.
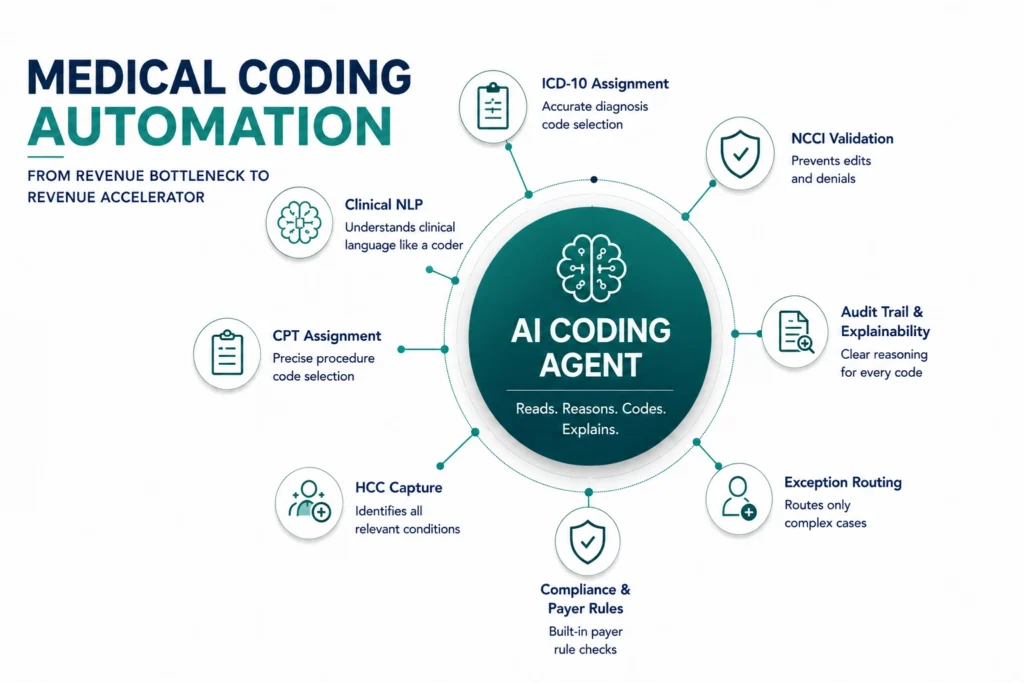
The fix is not another rules engine bolted onto an EHR. It is a category of software that can read a chart the way a coder reads it, decide the way a coder decides, and explain itself the way a coder would in an audit. That is what AI medical coding agents are built to do, and it is why 2026 is the year medical coding automation stopped being optional infrastructure and started becoming a competitive advantage. Unlike traditional medical coding software, modern AI agents can automate chart review, code assignment, validation, and audit preparation with minimal human intervention.
The 2026 Shift: Computer-Assisted Coding Software to Autonomous Medical Coding Agents
Traditional computer-assisted coding software suggested codes. Today’s autonomous medical coding systems powered by AI coding agents can assign, validate, and defend codes with significantly less human involvement.
For over a decade, CAC tools highlighted likely codes inside the chart and left a human to confirm every one. That model caps how fast any team can move, because the human is still the bottleneck on every single chart, no matter how good the underlying suggestion engine is.
In 2026, autonomous AI agents read unstructured clinical notes using advanced clinical NLP and large language models in healthcare, reasoning across ICD-10 codes, CPT procedures, and HCC categories simultaneously, while cross-checking NCCI edits and payer rules before submission.
The result sits on top of, not in place of, existing clinical workflows. The shift is not faster than CAC. It is a different division of labor between people and software, and it is part of a broader move toward agentic AI workflows across the revenue cycle, not just at the coding step.
Why Hospitals and Health Systems Are Moving First
For hospitals, the cost of slow or incomplete coding is measured in days of A/R and missed risk-adjustment revenue.
Inpatient coding complexity has risen more than 30% under stricter documentation requirements, and certified coder shortages mean backlogs of 10 to 45 days are common. This is one symptom of a wider staffing problem; the same pressure shows up across nursing, scheduling, and intake, which is why more health systems are now looking at how AI helps healthcare overcome staffing shortages as a system-wide strategy rather than a department-by-department fix.
AI agents drop validated codes into Epic or Cerner within minutes of discharge, directly cutting Days in A/R. The same logic extends downstream: once a chart is coded correctly, AI agents for accounts receivable can act on it immediately instead of waiting in a separate queue for a human to route the claim forward.
For value-based care contracts, agents scan complete clinical narratives for every relevant comorbidity, supporting adherence to HCC coding guidelines while improving the accuracy of retrospective risk adjustment initiatives. Every missed HCC represents lost reimbursement opportunities.
“An AI agent that explains every code it assigns is easier to defend in an audit than a coder’s memory from three months ago.”
Why Independent Practices and Groups Cannot Run on One Coder Anymore
A single coder out sick can freeze a small practice’s entire cash flow.
Mid-sized practices often have no redundancy: one person leaves, claims stop moving. Worse, many physicians still self-code Evaluation and Management visits between patients, trading clinical time for paperwork instead of the patients in the waiting room.
Agentic AI automates professional-fee coding directly from the physician’s clinical narrative, functioning like an intelligent CPT code lookup and validation engine that continuously checks payer-specific requirements and NCCI edits before claim submission. When a claim does get questioned, AI agents for denial management can work the appeal using the same documentation trail the coding agent already generated, instead of a biller starting research from scratch.
Coding accuracy is also only as good as what happens before the visit. Practices that pair coding automation with AI agents for eligibility verification catch coverage and authorization issues before the appointment, not after the claim bounces. The result across both is fewer reworked denials, predictable reimbursement timing, and hours of clinical time handed back to the physician instead of the keyboard.
Operational Leverage: Why RCM and Billing Companies Are Scaling Without Scaling Headcount
Margins in medical billing compress every year while clients demand faster, cleaner turnarounds.
RCM firms compete on cost and speed at the same time, which is structurally difficult with a fully manual coding workforce. Autonomous agents now process 70 to 80% of routine outpatient charts end to end, freeing human coders to focus entirely on exceptions, denial appeals, and audit defense, the work that actually needs judgment. Many firms are extending the same model downstream through AI agents for claim processing, broader claims processing automation, and AI-driven reimbursement workflows, enabling greater levels of revenue cycle management automation across the organization.
That shift also solves a growth problem. Winning a large new hospital account used to mean three to six months recruiting and training a regional coding team. With agentic capacity, RCM companies scale chart volume instantly instead of on a hiring timeline, which is the same logic behind broader AI agents for revenue cycle management adoption: the constraint shifts from headcount to configuration.
Scale Coding Capacity Without Scaling Headcount
Reduce chart backlog, improve coding throughput, and accelerate reimbursement with AI agents built for healthcare revenue cycle operations.
Trust Compliance: Why Audit Defensibility Is the Real Differentiator
Every buyer asks the same question eventually: what happens when a payer or regulator challenges a code?
A coder’s justification lives in their head and fades with time. An agent’s justification is written down at the moment the code is assigned, tied directly to the source documentation. That difference matters more as AI compliance oversight in healthcare becomes a standing requirement rather than an annual exercise, and it is also why coding automation cannot be evaluated on accuracy alone.
Because clinical documentation includes protected health information at every step, organizations evaluating AI medical coding solutions must ensure that the underlying architecture meets healthcare security, compliance, and auditability requirements.
That means real HIPAA-compliant AI architecture, not a generic model wrapped in a healthcare-sounding interface, and a deliberate approach to reducing AI-related compliance risk at the infrastructure level rather than the policy level alone.
Traditional Coding Tools vs Agentic AI, Side by Side
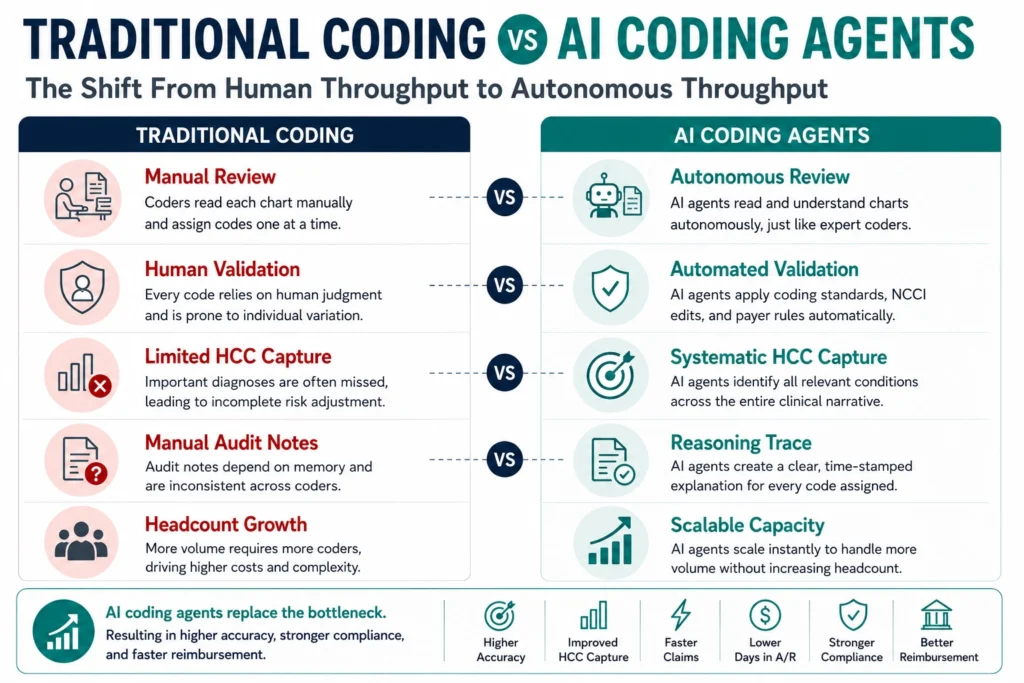
The difference between traditional medical coding software and modern agentic coding platforms is not speed alone. It is what each system can be trusted to do without requiring continuous human intervention.
| Traditional CAC | Agentic AI |
| Suggests codes; human confirms each one | Assigns and validates codes autonomously |
| No payer-rule check before submission | Cross-checks NCCI edits and payer rules pre-submission |
| Coder reviews every chart | Coders handle only flagged exceptions |
| Audit trail relies on manual chart notes | Built-in reasoning trace generated per code |
| Scaling means hiring more coders | Scaling means adding capacity on demand |
| HCC capture depends on reviewer attention | HCC capture is systematic across every chart |
Frequently Asked Questions
Medical coding automation uses software and AI to translate clinical documentation into standardized code sets such as ICD-10 codes, CPT procedures, and HCC categories without requiring manual chart review for every encounter. The newest systems use autonomous AI agents that read unstructured notes, assign and validate codes, and check payer rules before a claim is even submitted.
Older computer-assisted coding software primarily suggested codes. Modern AI coding agents can understand documentation context, apply coding logic, validate payer requirements, and escalate only exceptions that require human judgment.
Yes. AI coding agents support retrospective risk adjustment efforts by identifying documented conditions that align with HCC coding guidelines, helping organizations improve risk-score accuracy and reimbursement capture.
Agentic systems generate a reasoning trace for every code, showing exactly which documentation supported the decision. This gives compliance teams a clear, reviewable audit trail, generally stronger than relying on a human coder’s memory of why a code was chosen months earlier.
Most organizations connect an agent to their existing EHR and start on a limited chart volume within a few weeks, then expand once first-pass accuracy is validated against their own payer mix. Full-scale rollout timing depends more on internal review processes than on the technology itself.
See How AI Agents Improved Revenue Cycle Performance
Explore how healthcare organizations used AI agents to streamline coding workflows, reduce manual effort, and improve reimbursement outcomes across RCM.